Global monitoring of the WHO ‘25 by 25’ target

Global monitoring of the
WHO ‘25 by 25’ target
- proposal from the
Section of Cancer Information
Freddie Bray

WHO target - IARC proposal
•Global target to reduce premature
mortality from all NCDs by 25% by 2025
(4 key NCDs, ages 30-69)
•Proposal:
–Evaluate national cancer mortality trends
against the ‘25 by 25’ target
•Quantify whether the reduction is attainable
based on recent trends via prediction models
•Deliver a report card on cancer control progress
at the national and global level

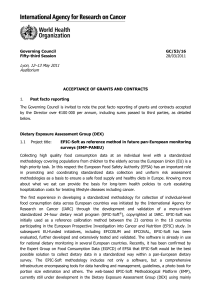
Data sources and availability
•Mortality extracted from the WHO mortality
database by country, cancer site, year, sex, age
•Data available for ≥15 years:
–78 countries
(35 Europe, 25 Americas, 15 Asia, 2 Oceania, 1 Africa)
•Data available for <15 years:
–8 countries
(4 Asia, 2 Europe, 2 Africa)
•Quality (coverage, completeness, timeliness)

National mortality series: availability

Methods
•Standard prediction models fitted to recent trends
(e.g. 1991-2010) to predict mortality 2011-2025
• National data available for ≥15 years:
–Age-period-cohort models based on a 15- or
20-year prediction base: NORDPRED (Moller et al, 2003)
•National data available for <15 years:
–Time-linear models based on a 10-year prediction
base (e.g. Dyba & Hakulinen, 1997)
• Future ‘all sites’ burden derived from site-specific
analyses (top ten cancers + residual sites by sex)
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
1
/
71
100%