Médecine personnalisée les questions actuelles Ce qui est simple

22/06/2015
1
Deauville 10 6 2015
Médecine personnalisée
les questions actuelles
Jean-Yves Blay
(Lyon, CLB, CRCL, U 1052, Eq 11)
LYRIC INCa 4664, DevWECAN, NetSARC, RREPS
Eurosarc FP7-278742
French Sarcoma Group
EORTC
Ce qui est simple est toujours
faux.
Ce qui ne l'est pas est
inutilisable.
(Paul Valéry)

22/06/2015
2
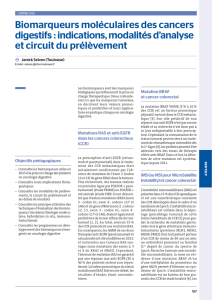
Sujets
• Hétérogénéité tumorale
• Drivers?
• Héterogénéité du stroma
• Thérapeutique
Learning More in the 20
th
Century
Leukemias,
Blood
Cancers
Breast
Lung
Cancer Colon
Cancer
Prostate
C
Cancer
C
ancer Other
Cancers,
including
Sarcomas
Appreciating the Complexity of Cancers
in the 21
st
Century

22/06/2015
3
Deauville 10 6 2015
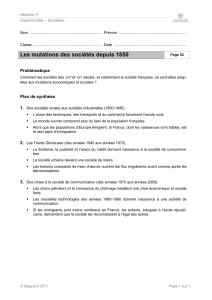
GIST
Mutations
kinases
WD/DDLPS
Amplification
12q13-15
MDM2/CDK4 TSG loss
NF1, TSC1/2
GIST
Sarcomas and
aggressive connective
tissue tumors
Ntl
Group
Tlti
MPNST
PEComas
Multiples niveaux Multiples niveaux
d’hétérogénéitéd’hétérogénéité
T
rans
l
oca
ti
ons
DFSP
SyS
Ewing
Mutations
APC/bCat
Desmoids
Genomique
complexe
LMS, UPS

22/06/2015
4
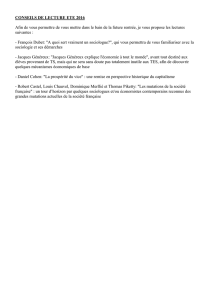
ESMO 2014
P. P. CassierCassier, , O.TrédanO.Trédan, C. , C. SeigneSeigne, E. , E. LavergneLavergne, J. Fayette, F. , J. Fayette, F. DesseigneDesseigne, P. , P. BironBiron, C. de la , C. de la FouchardièreFouchardière, I. , I. RayRay--CoquardCoquard, M. Pérol, D. , M. Pérol, D. FrappazFrappaz, M. , M.
BernardinBernardin, Q. Wang, V. , Q. Wang, V. AttignonAttignon, D. , D. PissalouxPissaloux, V. , V. CombaretCombaret, V. , V. AgrapartAgrapart, M.E. , M.E. FondrevelleFondrevelle, D. Pérol, J.Y. , D. Pérol, J.Y. BlayBlay, Centre Léon , Centre Léon BérardBérard, 28 rue , 28 rue
Laennec, Lyon, FranceLaennec, Lyon, France
IdentifyingIdentifying actionableactionable targetstargets in in advancedadvanced cancer patients: cancer patients:
PreliminaryPreliminary resultsresults fromfrom the the ProfiLERProfiLER program.program.
N=1590 patients as of N=1590 patients as of JuneJune 2015 (single center)2015 (single center)
ESMO 2014
IdentifyingIdentifying actionableactionable targetstargets in in advancedadvanced cancer cancer
patients: patients: PreliminaryPreliminary resultsresults fromfrom the the ProfiLERProfiLER
program.program.

22/06/2015
5
De multiples niveaux de complexité (1): Génomique
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
1
/
32
100%