MSI test - Oncomip

This could be the poster title
The molecular tests in colorectal cancer (KRAS, MSI):
Evaluation of practices in a large observational French cohort
J.MEILLEROUX (1), K. GORDIEN (2), E. OUM-SACK (2), M. AMARA KPOGHOMOU (2), P.GROSCLAUDE (3), J. GODDARD (2), J-P. MERLIO (4), I. SOUBEYRAN (5), R. GUIMBAUD (6),
V. BOUSSER (7), L. DIGUE (7), J SELVES (1).
(1) Service d’Anatomie et Cytologie Pathologiques, Pôle IUC Oncopole CHU, Institut Universitaire du Cancer de Toulouse - Oncopole, 1 avenue Irène Joliot-Curie - 31059 Toulouse cedex 9- France.
(2) Inserm U1027 : Epidémiologie et analyses en santé publique : risques, maladies chroniques et handicaps, Faculté de Médecine, 37 allées Jules Guesde, 31073 Toulouse, France
(3) Réseau régional de Cancérologie Oncomip, Institut Universitaire du Cancer de Toulouse - Oncopole, 1 avenue Irène Joliot-Curie - 31059 Toulouse cedex 9- France.
(4) Service d’Anatomie et de Cytologie Pathologiques, CHU Bordeaux, Hôpital Haut-Lévêque, Avenue de Magellan, 33604 Pessac cedex. France.
(5) Service d’Anatomie et de Cytologie Pathologiques, Institut Bergonié, 229 cours de l'Argonne - CS 61283 – 33076 Bordeaux Cedex, France
(6) Service de Cancérologie / Pôle Digestif et Oncogénétique (CHU Toulouse et Institut Claudius Regaud) Tumeurs digestives, 1 avenue Irène Joliot-Curie - 31059 Toulouse cedex 9, France.
(7) Réseau régional de cancérologie d’Aquitaine, 229 cours de l’Argonne 33076 Bordeaux, France.
Background
In addition of the morphological and the histo-prognostic factors evaluation in
colorectal cancer (CRC) specimen, the pathologist is now involved in the
analysis of molecular biomarkers. These are in CRC the screening of KRAS
mutation for metastatic patients which is mandatory for anti-EGFR treatment
and the evaluation of MSI (Microsatellite Instability) for Lynch syndrome
diagnosis.
The objective of this work was to evaluate the real-life practices of these
molecular tests and their therapeutic implications in general population of a
large French territory in 2010.
Methods
This work was performed from an observational survey conducted by
epidemiologists in two French regions (Midi-Pyrénées and Aquitaine) and
included 2,067 patients consecutively treated for a CRC in 2010. For each
patient, clinical, histological and therapeutic data were collected to create an
exhaustive data base.
Evaluation of molecular testing : KRAS mutation and MSI test
Molecular data were retrospectively collected from the 3 regional molecular
genetic centers and implemented in the database.
The molecular testing and his therapeutic implication in general population
was compared with the guidelines available in France in 2010.
Results
Conclusion
In 2010, the indications of the molecular tests were insufficiently respected.
The MSI test was performed only in 9 % of the population as opposed to 20 -
25% expected. These results make discuss the question of a large screening,
based on immunohistochemistry rather than molecular biology for Lynch
syndrome screening. The KRAS test was performed only in 68 % of metastatic
patients in 2010 but it widely improved during the last years (90 % in France in
2013*). Less than half patients eligible for anti-EGFR (no KRAS mutation) had
this targeted therapy at first line. A few no metastatic patients (essentially
stage III patients with poor prognosis factors) had KRAS test, which could
corresponds to anticipated test.
The role of these biomarkers (RAS, MSI) but also BRAF as prognostic factors for
stage II-III patients is widely demonstrated, but their place in routine practice
is not recommended to date.
KRAS mutation
a) KRAS mutation
French guidelines in 2010 :
- The test was recommended for each CRC metastatic patient to guide
chemotherapy and treatment.
- Only exon 2 KRAS testing was required.
The test was centralized in the regional molecular genetic centers (labelled by
the French National Cancer Institute, INCa).
Were evaluated : the number of KRAS tests performed for the whole
population (metastatic patients at diagnosis or not), and for patients
eligible for anti-EGFR (no KRAS mutation) the effective anti-EGFR
prescription (during the 6 months after the diagnosis).
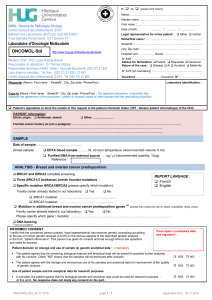
b) MSI Test
French guidelines in 2010 in CRC :
- Any patients with CRC diagnosis before 60 years age,
-Or patients with CRC and a personal or familial history at the 1st degree
of a tumor of Lynch syndrome,
- Any CRC with histological characteristics : tumor of the right colon,
undifferenciated, mucinous or single ring cells tumor.
Only MSI tests performed by molecular biology were collected from the 3
regional molecular genetic centers as recommended at this date in France.
Were evaluated : the number of MSI tests performed for the whole
population, and the association between the MSI test and the criteria
of the guidelines.
KRAS mutation was performed for 376/553 (68%) metastatic patients
(M+) and for 152/1421 (11%) no metastatic patients.
Among the 376 patients M + who had a test, 57 % had not exon 2
mutation, and was eligible to a treatment by anti-EGFR. Among these,
only 35 % (74) received the treatment as first line therapy.
Among the 152 no metastatic patients who had a test, the tumor
had poor prognostic factors in multivariate analysis (involved nodes
(p=0.0001), high level of tumoral infiltration pT4 (p= 0.003) or neo-
adjuvant treatment (p=0.011)).
MSI test
The MSI test was performed in 9% of the population of the study.
Only 40% patients of less than 60 years had a test.
Nowack et al, Cancer Epidemiol Biomarkers Prev; 24(9); 1416–8. 2015 AACR
1
/
1
100%