Syndrome inflammatoire et CEC A Ouattara Partie 1 bis

1
Pr Alexandre OUATTARA
Service d
’
Anesthésie Réanimation II, Hôpital du Haut-Lévêque,
Pôle d
’
Anesthésie-Réanimation, Groupe Hospitalier Sud, CHU de Bordeaux
Adaptation Cardiovasculaire à l
’
ischémie (Unité INSERM 1034)
Syndrome
inflammatoire en
chirurgie cardiaque
1
Agression tissulaire
Contexte infectieux ou non !
Réponse cellulaire Réponse humorale
SIRS = Systemic inflammatory Response Syndrome
Laffey JG et al. Anesthesiology 2002;97:215-52
Syndrome inflammatoire
Agression tissulaire
Contexte infectieux ou non infectieux
Réponse cellulaire Réponse humorale
SIRS = Systemic inflammatory Response Syndrome
ALI
Acute Lung Injury
Shock ARF
Acute Renal Failure
MODS
Multiple Organ
Dysfunction Syndrome
??
Laffey JG et al. Anesthesiology 2002;97:215-52
Réaction inflammatoire systémique
et chirurgie cardiaque
Expression biologique plus ou moins forte
(CRP, HL, fibrinogénémie…)
Expression clinique variable
Rougé P, Philip I. Congrès Français de Perfusion, Caen 2004
Prédisposition génétique, cercle vicieux entretenu
par dysfonction d’organes liée à hypoperfusion

2
Facteurs initiateurs de la réponse
inflammatoire
• Contact du sang à des surfaces étrangères (CEC)
• Hypoperfusion d’organes (intestinale+++)
– Translocation bactérienne
– Libération endotoxines
• Phénomènes d’ischémie-reperfusion d’organes
(cérébrale, cardiaque, pulmonaire, rénale et hépatique)
– Clampage aortique et hypoperfusion d’organes
– Reperfusion à l’origine d’une activation inflammatoire +++
Davies SW et al. J Thorac Cardiovasc Surg 1993; 105:979-87
Sawa Y et al. J Thorac Cardiovasc Surg 1996;111:29-35
La Circulation extra-corporelle (CEC)
Cardiac surgery/ Cardiopulmonary Bypass
Initiating Factors
•Contact Activation
•Complexe héparine-protamine
•Ischemia-Reperfusion
•Endotoxemia
Immune System Activation
•Complement
•Cytokines
•Coagulation/fibrinolysis
•Endothelium
•Cellular Immune System
SIRS
Interfaces Air – Sang – Matériel Activation de la voie du complément
* Anaphylatoxine
† complexe destructeur de la membrane
Etude expérimentale (cochons)
Impact de l’inhibition du C3 et C5 par solution soluble du Récepteur du complément de type 1 (CR1)
Sur la fonction cardiaque (travail myocardique=Preload Recruitable Systolic Work) et pulmonaire (RVP)
Chai PJ et al. Circulation 2000;101:541-6
CR1
C
C
CR1
Rinder CS, Rinder HM, Johnson K, Smith M, Lee DL, Tracey J, Polack G,
Higgins P, Yeh CG, Smith BR. Role of C3 cleavage in monocyte activation during
extracorporeal circulation. Circulation 1999; 100: 553-8
Park KW, Tofukuji M, Metais C, Communale ME, Dai HB, Simons M, Stahl GL,
Agah A, Sellke FW. Attenuation of endothelium-dependent dilation of pig
pulmonary arterioles after cardiopulmonary bypass is prevented by monoclonal
antibody to C5a. Anesth Analg 1999; 89: 42-8
Tofukuji M, Stahl GL, Agah A, Metais C, Simons M, Sellke FW. Anti-C5a
monoclonal antibody reduces cardiopulmonary bypass and cardioplegia-induced
coronary endothelial dysfunction. J Thorac Cardiovasc Surg 1998; 116: 1060-8
Tofukuji M, Stahl GL, Metais C, Tomita M, Agah A, Bianchi C, Fink MP, Sellke
FW. Mesenteric dysfunction after cardiopulmonary bypass: Role of complement
C5a. Ann Thorac Surg 2000; 69: 799-807
Gupta-Bansal R, Parent JB, Brunden KR. Inhibition of complement alternative
pathway function with anti-properdin monoclonal antibodies. Mol Immunol 2000;
37: 191-201
Larsson R, Elgue G, Larsson A, Ekdahl KN, Nilsson UR, Nilsson B. Inhibition of
complement activation by soluble recombinant CR1 under conditions resembling
those in a cardiopulmonary bypass circuit: Reduced upregulation of CD11b and
complete abrogation of binding of PMNs to the biomaterial surface.
Immunopharmacology 1997; 38: 119-27

3
Cardiac surgery/ Cardiopulmonary Bypass
Initiating Factors
•Contact Activation
•Complexe héparine-protamine
•Ischemia-Reperfusion
•Endotoxemia
Immune System Activation
•Complement
•
Cytokines
•Coagulation/fibrinolysis
•Endothelium
•Cellular Immune System
SIRS
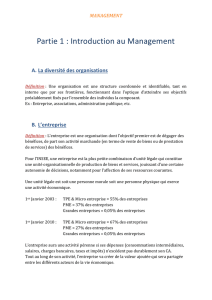
Interfaces Air – Sang – Matériel Cascade cytokinique au cours de la
chirurgie cardiaque
Polypeptides et protéines solubles
Messagers paracrines du système immunitaire
Produites par monocytes activés, macrophages tissulaires, lymphocytes, cellules
endothéliales…
Effet pro-inflammatoire (TNFalpha, IL-6) et anti-inflammatoire (IL-10)
Rôle majeur dans homéostasie immunologique (fine régulation)
Produite en réponse à des stimuli physiologique et/ou pathologique
Association statistique: taux élevé de cytokines et morbidité postopératoire
Relation de causalité entre cytokines et morbi-mortalité postopératoire (???)
Patient avec SIRS ont des taux de cytokines élevés
Taux d’IL-6 est corrélé avec la mortalité après chirurgie cardiaque pédiatrique
Libération de cytokines après chirurgie
cardiaque cardiaque
TNFα
IL-1β
IL6
IL8
IL-10
TGF b
IL-1ra
TNFsr 1 et 2
Pro-inflammatoire Anti-inflammatoire
Précoce
Tardive
Temp
s
[ ]°
C5a
TNFαIL1
IL6
Temps
Concentration
IL-10 est un puissant
inhibiteur de la production de
TNF-α, IL-1β, IL-6 et IL-8
Impact sur le pronostic
postopératoire dépend…
Pro-inflammatoire Anti-inflammatoire
McBride WT et al. Curr Opin Anaesth 1998;11:15-22

4
Cardiac surgery/ Cardiopulmonary Bypass
Initiating Factors
•Contact Activation
•Complexe héparine-protamine
•Ischemia-Reperfusion
•Endotoxemia
Immune System Activation
•Complement
•Cytokines
•
Coagulation/fibrinolysis
•Endothelium
•Cellular Immune System
SIRS
Interfaces Air – Sang – Matériel Interrelation surface artificielle / réactions de
défense non spécifique du sang = Phase contact
Phase Contact
Activation des différents systèmes protéiques plasmatiques
Coagulation Complément Fibrinolyse
• Synthèse de facteurs
antiplaquettaires puissants :
PGI2, NO
• Expression de la
Thrombomoduline (anti-ti-
coagulante)
• Libération de protéines
fibrinolytiques (t-PA)
Conditions physiologiques : la surface
vasculaire est anti-thrombogénique
PROCOAGULANT
ANTICOAGULANT
Les cytokines pro-inflammatoires, les translocation d’endotoxines
et d’autres facteurs d’agression induisent un état pro-coagulant
Au cours de l’inflammation…
PROCOAGULANT
ANTICOAGULANT
Surexpression du Facteur
tissulaire (FT), Plaminogen
activator inhibitor (PAI)-1 et
von Willebrand Factor (vWF)
Cardiac surgery/ Cardiopulmonary Bypass
Initiating Factors
•Contact Activation
•Complexe héparine-protamine
•Ischemia-Reperfusion
•Endotoxemia
Immune System Activation
•Complement
•Cytokines
•Coagulation/fibrinolysis
•
Endothelium
•Cellular Immune System
SIRS
Interfaces Air – Sang – Matériel Endothélium et syndrome inflammatoire

5
Cardiac surgery/ Cardiopulmonary Bypass
Initiating Factors
•Contact Activation
•Complexe héparine-protamine
•Ischemia-Reperfusion
•Endotoxemia
Immune System Activation
•Complement
•Cytokines
•Coagulation/fibrinolysis
•Endothelium
•
Cellular Immune System
SIRS
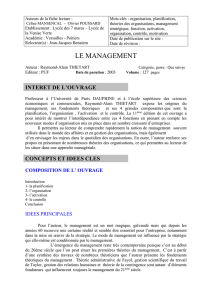
Interfaces Air – Sang – Matériel Réponse immunitaire cellulaire
Interaction Leucocytes / endothélium
•Séquestration pulmonaire +++
•Intérêt des stratégies de déplétion leucocytaire ?
Système immunitaire cellulaire et CEC
• Rôle majeur
• Activation des monocytes et macrophages
• Augmentation molécules d’adhésion (sélectines et
intégrines)
• Génération de radicaux libres Figure 1. Pathophysiology of two-hit mediated
transfusion-related acute lung injury (TRALI)
Panel 1. Definition of transfusion-related acute
lung injury (TRALI)
Suspected TRALI
• Acute onset within 6 h of blood transfusion
• PaO2/FIO2<300 mm Hg or worsening P/F ratio
• Bilateral infiltrative changes on chest graph
• No sign of hydrostatic pulmonary oedema
(PCWP ≤18 mm Hg or CVP≤15 mm Hg)
• No other risk factor for acute lung injury
Possible TRALI
Same as for suspected TRALI, but another risk
factor present for acute lung injury
Delayed TRALI
Same as for (possible) TRALI and onset within 6–
72 h of blood transfusion
Transfusion-related acute lung injury: a clinical review
Alexander P J Vlaar, Nicole P Juff ermans
Lancet 2013; 382: 984–94
Système
complément Cytokines
Coagulation/
fibrinolyse Immunité
cellulaire
Cellules
endothéliales
(NO)
SIRS in cardiac surgery
 6
7
8
9
10
6
7
8
9
10
1
/
10
100%