Cours DES Fausses couches

Produits de conception
Aurore Coulomb
Service d’Anatomie et Cytologie Pathologiques
Groupe Hospitalier A Trousseau – La Roche Guyon
DES d’Anatomie et Cytologie Pathologiques
Mardi 3 février 2009

Méthode d’examen
•Poids
•cavité ovulaire intacte
–taille
–embryon
•examen
•LCC
•nuque
–cordon
–vésicule vitelline
•débris : placenta, caduque, embryon
•caryotype (récidive de fausse couche)
•histologie : placenta, embryon, caduque
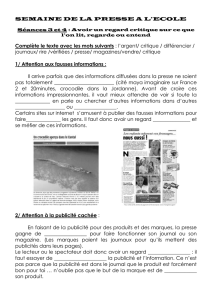
Vésicule
amniotique
Vésicule
vitelline

DEFINITIONS
DEFINITIONS
•Fausse couche spontanée
–perte embryo-foetale spontanée
•Fausses couches spontanées récidivantes
–nomenclature : fausse couche récurrente
–3 ou plus pertes spontanées [consécutives, non consécutives]
•primaire : pas de naissance vivante
•secondaire : fausses couches récidivante après naissance vivante
–Représentent 3% des fausses couches spontanées
•Fausse couche spontanée précoce
–avant 14 SA (1
er
trimestre)
•Fausse couche spontanée tardive FCT
–entre 14-20 SA (début 2
ème
trimestre, période pré viabilité; pour
certains auteurs jusqu’à 24 SA)

Fausses couches
Fausses couches
MECHANISMES
MECHANISMES
•MATERNELLE
–SYSTEMIQUE
•GENETIQUE (5%)
•IMMUNOLOGIQUE (5-25%)
•HORMONAL (20-40%)
–LOCAL
•ANATOMIQUE (10-20%)
•PATERNELLE
–SYSTEMIQUE (GENETIQUE) (Part of 5%)
•ENVIRONMENTAL
–TOXIQUE (Rare)
–INFECTIEUX (1-5%)
•INCONNU (20-60%)

FAUSSES COUCHES
FAUSSES COUCHES
MECHANISMES MATERNELS
MECHANISMES MATERNELS
•
SYSTEMIQUE
–GENETIQUE = CHROMOSOMIQUE
•anomalie gamétogenèse : non disjonction chromosomique
•translocations familiales déséquilibrées (5%)
PRE-MOM MERE PERE
BABY
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
1
/
35
100%