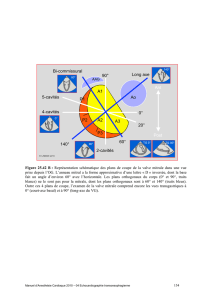
Hypertrophic Obstructive Cardiomyopathy

"And he said to me, you must have
made a mistake. I left the operating
room very humbled."
1959
Eugene Braunwald Andrew G. Morrow
1859 H. LIOUVILLE
Hypertrophic
Cardio
Myopathy

1-EH 4 0566 01 11/2010 2

Morrow Procedure (Sixties)

Morrow Procedure (Sixties)
« the incisions are made quite close to the seat of the soul »
5 / 10 gr

Morrow Procedure (Results)
 6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
1
/
36
100%